Quantitative Research Designs
The type of research design selected depends on whether the researcher aims to describe, explore relationships, or test interventions.
Quantitative research study designs can be broadly classified into two main groups (observational and experimental) depending on if an intervention is assigned. If an intervention is assigned, then an experimental study design will be considered; however, if no intervention is planned or assigned, then an observational study will be conducted. These broad classes are further subdivided into specific study designs, as shown in Figure 8.1. In practice, quantitative studies usually begin simply as descriptive studies, which could subsequently be progressed to more complex analytic studies and then to experimental studies where appropriate.
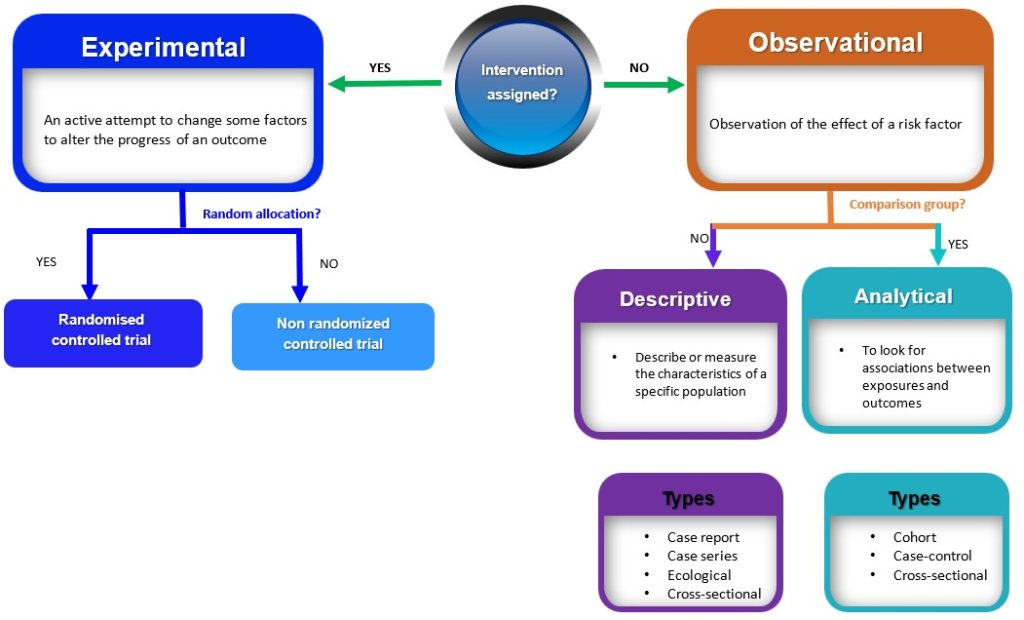
Figure 8.1 Algorithm for classification of study designs by Bunmi Malau-Aduli and Faith Alele. Adapted from Grimes and Schulz 2002, used under a CC BY NC 4.0 license.
Observational Study Designs
In many nursing studies, interventions cannot ethically be assigned, such as when studying smoking or stress, making observational designs essential tools for understanding associations without manipulation. Observational studies are research designs that involve observing and measuring the characteristics of a sample or population without intervening, altering or manipulating any variables (Figure 8.1). Observational studies can be further subdivided into descriptive and analytic studies.
 Dr. Fehr Tip:
Dr. Fehr Tip:
We often use observational studies in nursing when interventions can’t ethically or practically be assigned, for example, studying patient outcomes after natural disasters.
Descriptive observational studies
Descriptive studies are research designs that describe or measure the characteristics of a specific population or phenomenon. These characteristics include descriptions related to the phenomenon under investigation, the people involved, the place, and the time. These study designs are typically non-experimental and do not involve manipulating variables; rather, they rely on the collection and analysis of numerical data to draw conclusions. Examples of descriptive studies include case reports, case series, ecological studies and cross-sectional (prevalence studies).
Once a descriptive study identifies patterns or possible risk factors, researchers often move toward analytic designs, such as case-control or cohort studies, to explore whether these patterns represent causal relationships.
Case Reports and Case Series
Case reports and case series are both types of descriptive studies in research. A case report is a detailed account of the medical history, diagnosis, treatment, and outcome of a single patient. On the other hand, case series is a collection of cases with similar clinical features. Case series are frequently used to explain the natural history of a disease, the clinical characteristics, and the health outcomes for a group of patients who underwent a certain treatment. Case series typically involve a larger number of patients than case reports. Both case reports and case series are used to illustrate unusual or atypical features found in patients in practice. In a typical, real-world clinical situation, they are both used to describe the clinical characteristics and outcomes of individual patients or a group of patients with a particular condition. These studies have the potential to generate new research questions and ideas.
However, there are drawbacks to both case reports and case series, such as the absence of control groups and the potential for bias. Yet, they can be useful sources of clinical data, particularly when researching uncommon or recently discovered illnesses. An example of a case report is the study by van Tulleken, Tipton and Haper, 2018 which showed that open-water swimming was used as a treatment for major depressive disorder for a 24-year-old female patient. Weekly open (cold) water swimming was trialed, leading to an immediate improvement in mood following each swim. A sustained and gradual reduction in symptoms of depression, and consequently a reduction in, and cessation of, medication was observed. An example of a case series is the article by Chen et al, 2020 which described the epidemiology and clinical characteristics of COVID-19 infection among 12 confirmed cases in Jilin Province, China.
Dr. Fehr Tip:
Case reports are often where nurses notice early warning signs that prompt larger studies, your clinical observation skills matter! Case reports also often spark the first new nursing interventions or identify early warning signs of adverse effects.
Case Report, Nursing Practice Example
A public health nurse documents the case of a 45-year-old man who developed severe skin irritation following the use of a new wound care dressing. The nurse’s detailed report of symptom progression, product use, and response to alternative treatments helps identify a potential product-related reaction.
Dr. Fehr Tip:
Case series can raise red flags about policy or procedural changes in a care unit, they’re often the first step in quality improvement research.
Case Series, Nursing Practice Example
A group of wound care nurses report on 10 long-term care patients who developed pressure injuries after a new repositioning schedule was implemented. The case series describes patient characteristics, wound stages, and outcomes, helping to highlight patterns in care needs and prevention strategies.
Ecological Studies
Ecological studies examine the relationship between exposure and outcome at the population level. Unlike other epidemiological studies focusing on individual-level data, ecological studies use aggregate data to investigate the relationship between exposure and outcome of interest. In ecological studies, data on prevalence and the degree of exposure to a given risk factor within a population are typically collected and analyzed to see if exposure and results are related. Ecological studies shed light on the total burden of disease or health-related events within a population and assist in the identification of potential risk factors that might increase the incidence of disease/event.
However, these studies cannot prove causation or take into account characteristics at the individual level that can influence the connection between exposure and result. This implies that ecological findings cannot be interpreted and extrapolated to individuals. For example, the association between urbanization and Type 2 Diabetes was investigated at the country level, and the role of intermediate variables (physical inactivity, sugar consumption and obesity) was examined. One of the key findings of the study showed that in high-income countries (HIC), physical inactivity and obesity were the main determinants of T2D prevalence. However, it will be wrong to infer that people who are physically inactive and obese in HIC have a higher risk of T2D.
Dr. Fehr Tip:
Ecological studies are great for examining population-level trends, but remember, they can’t tell you what’s happening with individuals.
Ecological Study, Nursing Practice Example
Nurse researchers examine provincial data comparing vaccination rates and influenza-related hospital admissions across Canadian regions. The study explores whether areas with higher nurse-led vaccination clinics have lower hospitalization rates for influenza.
Cross-Sectional Descriptive Studies
A cross-sectional study is an observational study in which the researcher collects data on a group of participants at a single point in time. The goal is to describe the characteristics of the group or to explore relationships between variables. Cross-sectional studies can be either descriptive or analytical (Figure 3.2). Descriptive cross-sectional studies are also known as prevalence studies measuring the proportions of health events or conditions in a given population. 11 Although analytical cross-sectional studies also measure prevalence, however, the relationship between the outcomes and other variables, such as risk factors, is also assessed.
The main strength of cross-sectional studies is that they are quick and cost-effective. However, they cannot establish causality and may be vulnerable to bias and confounding (these concepts will be discussed further later in this chapter under “avoiding error in quantitative research). An example of a cross-sectional study is the study by Kim et al., 2020 which examined burnout and job stress among physical and occupational therapists in various Korean hospital settings. Findings of the study showed that burnout and work-related stress differed significantly based on several factors, with hospital size, gender, and age as the main contributory factors. The more vulnerable group consisted of female therapists in their 20s at small- or medium-sized hospitals with lower scores for quality of life.
Dr. Fehr Tip:
Cross-sectional descriptive studies give a snapshot in time, helpful for identifying what’s common, but not why it happens.
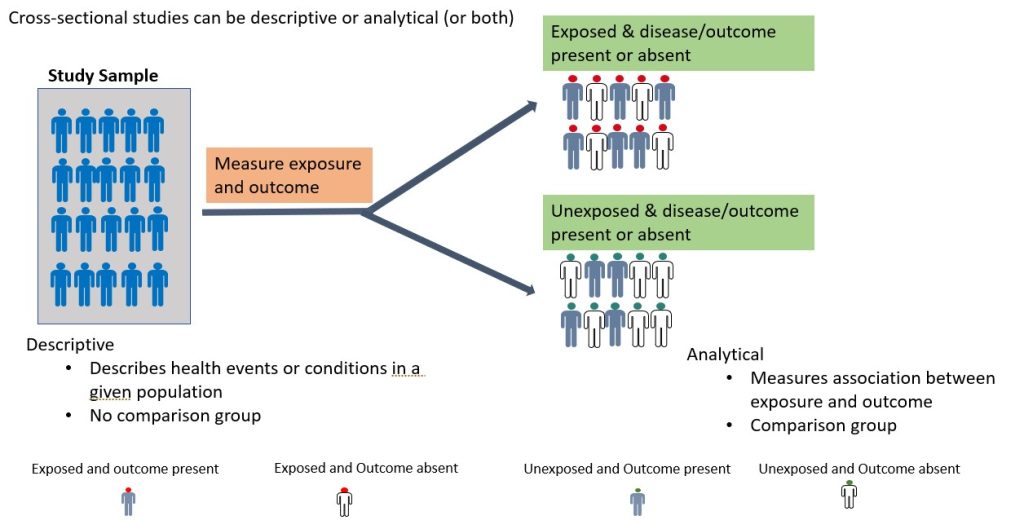
Figure 8.2 Cross-sectional studies by Bunmi Malau-Aduli and Faith Alele, used under a CC BY NC 4.0 licence.
Cross-Sectional Descriptive Study, Nursing Practice Example
A community health nurse conducts a survey of 500 adults in a rural area to determine the prevalence of hypertension and associated health behaviors such as diet and physical activity.
Analytical Observational studies
Analytical observational studies aim to establish an association between exposure and outcome and identify causes of disease (causal relationship). Analytical observational studies include analytical cross-sectional (discussed above), case-control and cohort studies. This research method could be prospective (cohort study) or retrospective (case-control study), depending on the direction of the enquiry.
Analytical Cross-Sectional Study, Nursing Practice Example
A nurse researcher surveyed 300 hospital nurses to explore the relationship between shift length and reported levels of fatigue and patient care errors. Statistical analysis shows that longer shifts are significantly associated with higher fatigue levels.
Dr. Fehr Tip:
These studies look at relationships between factors—keep in mind that relationships don’t always mean causation!
Case-Control Studies
A case-control study is a retrospective study in which the researcher compares a group of individuals with a specific outcome (cases) to a group of individuals without that outcome (controls) to identify factors associated with the outcome. As shown in Figure 8.3 below, the cases and controls are recruited and asked questions retrospectively (going back in time) about possible risk factors for the outcome under investigation. A case-control study is relatively efficient in terms of time, money and effort, suited for rare diseases or outcomes with a long latent period, and can examine multiple risk factors. For example, before the cause of lung cancer, was established, a case-control study was conducted by British researchers Richard Doll and Bradford Hill in 1950. Subjects with lung cancer were compared with those who did not have lung cancer, and details about their smoking habits were obtained. The findings from this initial study showed that cancer patients were more frequent and heavy smokers. Over the years, more evidence has been generated implicating tobacco as a significant cause of lung cancer. Case-control studies are, therefore, useful for examining rare outcomes and can be conducted more quickly and with fewer resources than other study designs. Nonetheless, it should be noted that case-control studies are susceptible to bias in selecting cases and controls and may not be representative of the overall population.
Dr. Fehr Tip:
Case-control studies work backward in time—useful when you’re studying rare events like workplace injuries or infections.
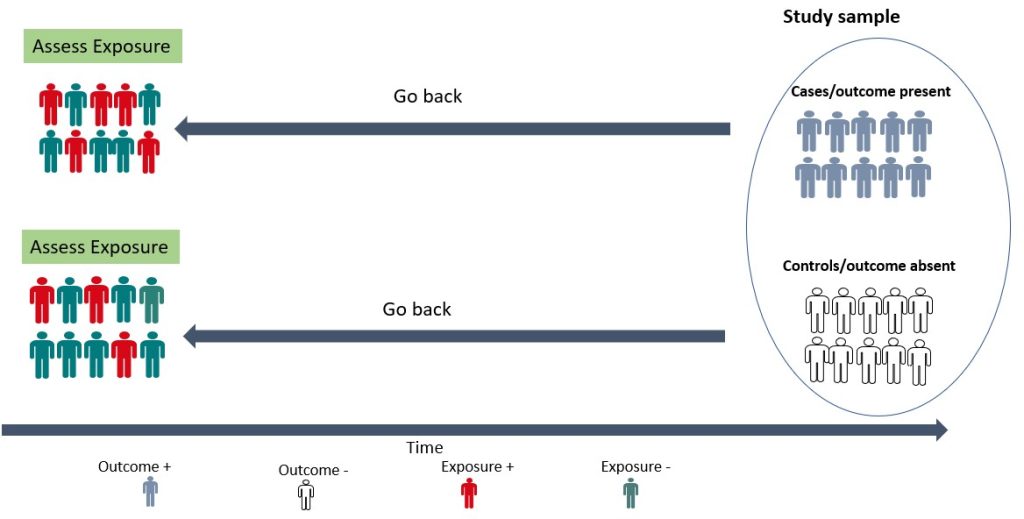
Figure 8.3 Case-Control studies by Bunmi Malau-Aduli and Faith Alele, used under a CC BY NC 4.0 licence.
Case-Control Study, Nursing Practice Example
Researchers compare nurses who experienced needle-stick injuries (cases) with those who have not (controls). They examine prior training in safe injection techniques, workload, and use of protective equipment to identify risk factors associated with the injuries.
Cohort Study
Cohort studies are longitudinal studies in which the researcher follows a group of individuals who share a common characteristic (e.g., age, occupation) over time to monitor the occurrence of a particular health outcome. The study begins with the selection of a group of individuals who are initially free of the disease or health outcome of interest (the “cohort”). The cohort is then divided into two or more groups based on their level of exposure (for example, those who have been exposed to a certain risk factor and those who have not). Participants are then followed up, and their health outcomes are tracked over time. The incidence of the health outcome is compared between exposed and non-exposed groups, and the relationship between exposure and the outcome is quantified using statistical methods.
Cohort studies can be prospective or retrospective (Figure 8.4). In a prospective cohort study, the researchers plan the study so that participants are enrolled at the start of the study and followed over time. In a retrospective cohort study, data on exposure and outcome are collected from existing records or databases. The researchers go back in time (via available records) to find a cohort that was initially healthy and “at risk” and assess each participant’s exposure status at the start of the observation period. Cohort studies provide an understanding of disease risk factors based on findings in thousands of individuals over many years and are the foundation of epidemiological research. They are useful for investigating the natural history of a disease, identifying risk factors for a disease, providing strong evidence for causality and estimating the incidence of a disease or health outcome in a population.
However, they can be expensive and time-consuming to conduct. An example of a cohort study is the study by Watts et al, 2014 which investigated whether the communication and language skills of children who have a history of stuttering are different from children who do not have a history of stuttering at ages 2–5 years. The findings revealed that children with a history of stuttering, as a group, demonstrated higher scores on early communication and language measures compared to their fluent peers. According to the authors, clinicians can be reassured by the finding that, on average, children who stutter have early communication and language skills that meet developmental expectations.
Dr. Fehr Tip:
Cohort studies are powerful for identifying risk factors—especially when following nurses or patients over time
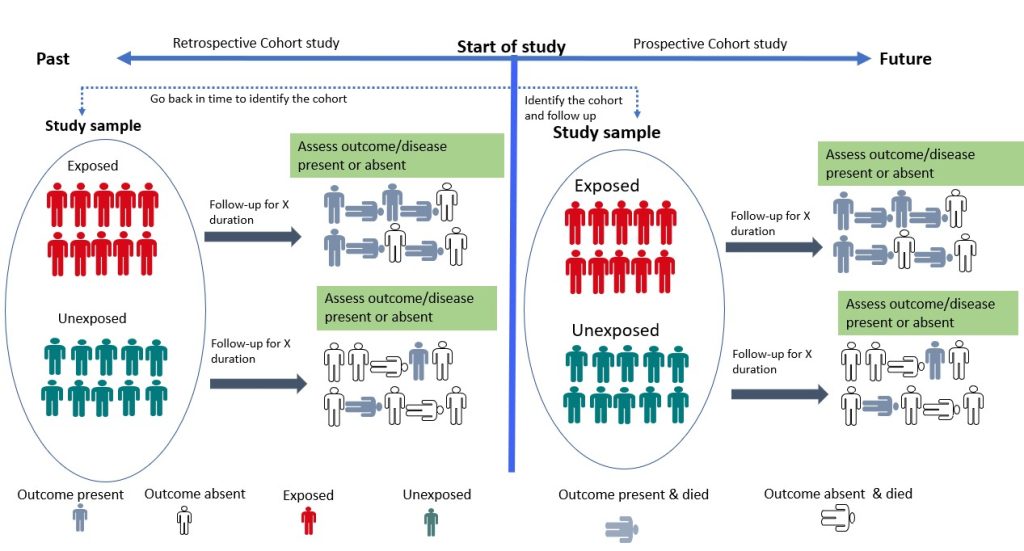
Figure 8.4 Cohort Studies by Bunmi Malau-Aduli and Faith Alele, used under a CC BY NC 4.0 licence
Cohort Study (Prospective or Retrospective), Nursing Practice Example
A team of occupational health nurses follows a group of 1,000 newly employed nurses for five years to examine whether consistent use of ergonomic lifting techniques reduces the incidence of musculoskeletal injuries compared to those who don’t use proper techniques.
Experimental Study Designs
While observational studies identify potential relationships, experimental studies allow researchers to test whether those relationships are truly cause and effect. Experimental studies involve manipulating one or more variables in order to measure their effects on one or more outcomes. In this type of study, the researcher assigns individuals to two or more groups that receive or do not receive the intervention. Well-designed and conducted interventional studies are used to establish cause-and-effect relationships between variables. Experimental studies can be broadly classified into two–randomized controlled trials and non-randomized controlled trials.
Dr. Fehr Tip:
If you want to test whether an intervention works, you’ll need an experimental design, but remember, feasibility and ethics come first.
Randomized Controlled Trial
Randomized controlled trials (RCTs) are experimental studies in which participants are randomly assigned to the intervention or control arm of the study. The experimental group receives the intervention, while the control group does not (Figure 8.5). RCTs involve random allocation (not by choice of the participants or investigators) of participants to a control or intervention group (Figure 8.5). Randomization or random allocation minimizes bias and offers a rigorous method to analyze cause-and-effect links between an intervention and outcome. Randomization balances participant characteristics (both observed and unobserved) between the groups. This is so that any differences in results can be attributed to the research intervention. The most basic form of randomization is allocating treatment by tossing a coin. Other methods include using statistical software to generate random number tables and assigning participants by simple randomization or allocating them sequentially using numbered opaque envelopes containing treatment information. This is why RCTs are often considered the gold standard in research methodology.
While RCTs are effective in establishing causality, they are not without limitations. RCTs are expensive to conduct and time-consuming. In addition, ethical considerations may limit the types of interventions that can be tested in RCTs. They may also not be appropriate for rare events or diseases and may not always reflect real-world situations, limiting their application in clinical practice. An example of a randomized controlled trial is the study by Shebib et al., 2019 which investigated the effect of a 12-week digital care program (DCP) on improving lower-back pain. The treatment group (DCP) received the 12-week DCP, consisting of sensor-guided exercise therapy, education, cognitive behavioural therapy, team and individual behavioural coaching, activity tracking, and symptom tracking – all administered remotely via an app. While the control group received three digital education articles only. The findings of the study showed that the DCP resulted in improved health outcomes compared to treatment-as-usual and has the potential to scale personalized evidence-based non-invasive treatment for patients with lower-back pain.
Dr. Fehr Tip:
RCTs are the gold standard, randomization helps ensure that any difference in outcomes is really due to your nursing intervention.
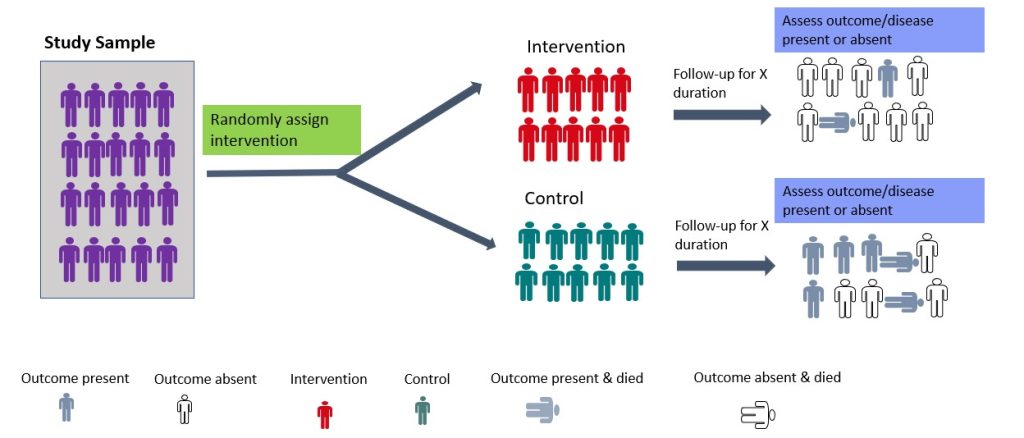
Figure 8.5 Schematic of experimental studies- randomised control trials by Bunmi Malau-Aduli and Faith Alele, used under a CC BY NC 4.0 licence.
Randomized Controlled Trial (RCT), Nursing Practice Example
A nurse-led research team randomly assigns post-surgical patients to either a mindfulness-based pain management intervention or standard care. The team measures pain intensity and anxiety levels over four weeks. The results show a statistically significant reduction in pain and anxiety for those in the intervention group.
Non-Randomized Controlled Design
Non-randomized controlled trial (non-RCT) designs are used where randomization is impossible or difficult to achieve. This type of study design requires allocation of the exposure/intervention by the researcher. In some clinical settings, it is impossible to randomize or blind participants. In such cases, non-randomized designs are employed. Examples include pre-posttest design (with or without controls) and interrupted time series. For the pre-posttest design that involves a control group, participants (subjects) are allocated to intervention or control groups (without randomization) by the researcher. On the other hand, it could be a single pre-posttest design study where all subjects are assessed at baseline, the intervention is given, and the subjects are re-assessed post-intervention. An example of this type of study was reported by Lamont and Brunero (2018), who examined the effect of a workplace violence training program for generalist nurses in the acute hospital setting. The authors found a statistically significant increase in behaviour intention scores and overall confidence in coping with patient aggression post-test.
Another type of non-RCT study is the interrupted time series (ITS) in which data are gathered before and after intervention at various evenly spaced time points (such as weekly, monthly, or yearly). Thus, it is crucial to take note of the precise moment an intervention occurred. The primary goal of an interrupted time series is to determine whether the data pattern observed post-intervention differs from that noted prior. Several ITS were conducted to investigate the effectiveness of the different prevention strategies (such as lockdown and border closure) used during the COVID pandemic. Although non-RCT may be more feasible to RCTs, they are more prone to bias than RCTs due to the lack of randomization and may not be able to control for all the variables that might affect the outcome.
Dr. Fehr Tip:
When randomization isn’t possible, non-randomized trials can still provide strong practical evidence, especially in real-world hospital settings.
Descriptive cross-sectional: ‘What proportion of nurses experience burnout?’
Analytical cross-sectional: ‘Is burnout associated with shift length among nurses?’
Non-Randomized Controlled Trial, Nursing Practice Example
A hospital implements a new falls prevention program on one unit while another unit continues standard care. The nurse researcher compares fall rates before and after the intervention between the two units. Participants were not randomly assigned due to logistical reasons.
Reflection
Reflection Prompt:
Think of a recent nursing research article you have read (or one provided in class). Using what you’ve learned about quantitative designs and critical appraisal tools (like CASP or JBI):
Identify the type of quantitative study design used (e.g., cross-sectional, cohort, RCT).
Ask yourself:
- What makes this study credible or less trustworthy?
- Were there any potential biases or confounding factors?
- Are the findings relevant to your nursing practice or the population you work with?
Reflect on how this evidence could influence nursing decision-making, patient education, or policy development in your area of practice.
Hierarchy of Evidence
While each study design has its unique characteristics and strengths, they are not without weaknesses (as already discussed) that impact the accuracy of the results and research evidence they provide. Understanding where each design fits within the hierarchy of evidence helps nurses critically appraise literature and apply the most reliable findings to clinical decision-making. The hierarchy of evidence is a framework used to rank the evidence provided by different study designs in research evaluating healthcare interventions with respect to the strength of the presented results (i.e., validity and reliability of the findings). Study designs can be ranked in terms of their ability to provide valid evidence on the effectiveness (intervention achieves the intended outcomes), appropriateness (impact of the intervention from the perspective of its recipient) and feasibility (intervention is implementable) of the research results they provide.
As shown in Figure 8.6, meta-analyses, systematic reviews, and RCTs provide stronger best-practice evidence and scientific base for clinical practice than descriptive studies as well as case reports and case series. Nonetheless, it is important to note that the research question/ hypothesis determines the study design, and not all questions can be answered using an interventional design. In addition, there are other factors that need to be considered when choosing a study design, such as funding, time constraints, and ethical considerations.
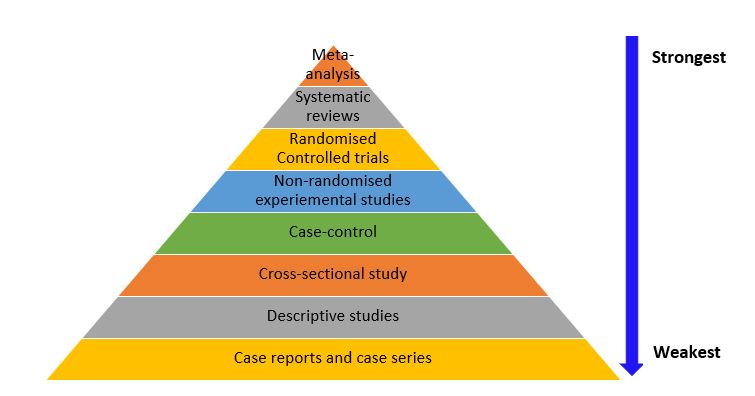
Figure 8.6 Hierarchy of Evidence by Bunmi Malau-Aduli and Faith Alele, adapted from Buettner 2015, used under a CC BY NC 4.0 licence
Activity
Critical Appraisal in Practice: Thinking Like a Nurse-Researcher
Understanding the hierarchy of evidence is only the first step in evaluating quantitative research. Nurses must also be able to critically appraise the quality and applicability of research studies before integrating findings into clinical practice. Critical appraisal involves systematically reviewing a study’s design, methods, data analysis, and conclusions to judge how trustworthy and relevant the results are.
Several frameworks help guide this process. The Critical Appraisal Skills Programme (CASP) provides structured checklists for evaluating quantitative studies such as randomized controlled trials, cohort studies, and case-control studies. Similarly, the Joanna Briggs Institute (JBI) offers evidence-based tools that help nurses assess the methodological quality and risk of bias in research articles. Using these frameworks allows nurses to identify strengths and weaknesses in research design and determine whether the evidence can be confidently applied to patient care.
Critical Appraisal in Practice: Thinking Like a Nurse-Researcher
Example scenario:
A nurse researcher reads a randomized controlled trial (RCT) that tests whether a nurse-led mindfulness program reduces anxiety in post-surgical patients compared to standard care. The study reports a statistically significant reduction in anxiety levels in the intervention group.
Using the CASP RCT Checklist, a critical appraisal might include:
- Was the trial randomized properly?
Answer: The study describes computer-generated randomization, which helps minimize bias.
- Were all participants accounted for?
Answer: Of 120 patients enrolled, 10 dropped out before completion. The researchers used intention-to-treat analysis to include all participants, which maintains validity.
- Were participants and researchers blinded?
Answer: The mindfulness facilitator knew which group participants were in, but outcome assessors did not—partial blinding, which can still limit bias.
- How large was the treatment effect, and is it clinically meaningful?
Answer: The intervention group’s anxiety scores decreased by 25%, but the clinical importance depends on how this translates to patient comfort and recovery.
- Can the results be applied to my nursing setting?
Answer: If your hospital serves similar post-surgical populations, the findings could inform the development of a nurse-led anxiety-reduction program.
Dr. Fehr Tip:
As a nurse, you’ll often use the hierarchy of evidence to decide which findings to trust most when applying research to patient care.
Remixed from:
- Scientific Inquiry in Social Work by Matthew DeCarlo (2018) published by pressbooks under a CC BY-NC-SA license.
Media Attributions
- Dr. Fehr [avatar] by Research Assistant Katie Gregson on Canva using Canva AI image creation https://www.canva.com/ai-assistant/ is subject to the Canva Pro Content License.
References
DeCarlo, M. (2018). Chapter 3: “Navigating quantitative research”. In Scientific Inquiry in Social Work. Pressbooks. https://jcu.pressbooks.pub/intro-res-methods-health/part/3-navigating-quantitative-research/
Doll, R., & Hill, A. B. (1950). Smoking and Carcinoma of the Lung. BMJ, 2(4682), 739–748. https://doi.org/10.1136/bmj.2.4682.739
Du, N., Chen, H., Zhang, Q., Che, L., Lou, L., Li, X., Zhang, K., & Bao, W. (2020). A case series describing the epidemiology and clinical characteristics of COVID-19 infection in Jilin Province. Virulence, 11(1), 482–485. https://doi.org/10.1080/21505594.2020.1767357
Kim, J.-H., Kim, A.-R., Kim, M.-G., Kim, C.-H., Lee, K.-H., Park, D., & Hwang, J.-M. (2020). Burnout Syndrome and Work-Related Stress in Physical and Occupational Therapists Working in Different Types of Hospitals: Which Group Is the Most Vulnerable? International Journal of Environmental Research and Public Health, 17(14), 5001. https://doi.org/10.3390/ijerph17145001
Lamont, S., & Brunero, S. (2018). The effect of a workplace violence training program for generalist nurses in the acute hospital setting: A quasi-experimental study. Nurse Education Today, 68, 45–52. https://doi.org/10.1016/j.nedt.2018.05.008
Shebib, R., Bailey, J. F., Smittenaar, P., Perez, D. A., Mecklenburg, G., & Hunter, S. (2019). Randomized controlled trial of a 12-week digital care program in improving low back pain. Npj Digital Medicine, 2(1). https://doi.org/10.1038/s41746-018-0076-7
van Tulleken, C., Tipton, M., Massey, H., & Harper, C. M. (2018). Open water swimming as a treatment for major depressive disorder. BMJ Case Reports, bcr-2018-225007. https://doi.org/10.1136/bcr-2018-225007
Watts, A., Eadie, P., Block, S., Mensah, F., & Reilly, S. (2014). Language ability of children with and without a history of stuttering: A longitudinal cohort study. International Journal of Speech-Language Pathology, 17(1), 86–95. https://doi.org/10.3109/17549507.2014.923512
Research that is non-experimental because it focuses on recording systemic observations of behavior in a natural or laboratory setting without manipulating anything.
A study design that tests whether a specific intervention or treatment causes a change in an outcome
Case reports and case series are both types of descriptive studies in research. A case report is a detailed account of the medical history, diagnosis, treatment, and outcome of a single patient. Case series are used to explain the natural history of a disease, the clinical characteristics, and the health outcomes for a group of patients who underwent a certain treatment.
Ecological studies examine the relationship between exposure and outcome at the population level. Data on prevalence and the degree of exposure to a given risk factor within a population are usually collected and analyzed to see if exposure and results are related. Ecological studies shed light on the total burden of disease or health-related events within a population and assist in identifying potential risk factors that might increase the incidence of disease/event.
Cross-sectional studies are observational studies in which the researcher collects data on a group of participants at a single point in time. The goal is to describe the characteristics of the group or to explore relationships between variables. Cross-sectional studies can be either descriptive or analytical.
Cohort studies are longitudinal studies where a researcher follows a group of individuals who share a common characteristic (e.g., age, occupation) over time to monitor the occurrence of a particular health outcome. Study begns with selecting a group of people initially free of the health outcome, then the cohort is divided into groups based on their level of exposure to a risk factor. Participants are then followed up and health outcomes tracked over time. Cohort studies can be prospective or retrospective.
A case-control study is a retrospective study in which the researcher compares a group of individuals with a specific outcome (cases) to a group of individuals without that outcome (controls) to identify factors associated with the outcome.
Randomized control trials (RCTs) are experimental studies in which participants are randomly assigned to the intervention or control aim of the study. The experimental group receives the intervention, while the control group does not. RCTs involve random allocation of participants to a control or intervention group. Randomization balances participant characteristics between the groups.
Non-randomized controlled trial (non-RCT) designs are used where randomization is impossible or difficult to achieve. This type of study design requires allocation of the exposure/intervention by the researcher.
The process of carefully examining a research study to determine whether its methods and findings are trustworthy and useful